

Opioids
- Team: Jeffrey K Aronson, Ben Goldacre, Carl Heneghan, Kamal R. Mahtani
- Theme: Therapeutics
- Completed projects
 ©
Shutterstock
©
Shutterstock
Since the 1990s, the prescribing of strong pain medicines called opioids has increased in England and most high-income countries. Oxford researchers review the global and national use of opioids and have developed tools to improve patient safety. The core areas of research and their outputs are highlighted below.
Global use of opioids
Previous studies of global opioid use have concentrated on morphine alone or a subset of opioids, with a focus on cancer pain and palliative care. We conducted a cross-sectional study using data from the International Narcotics Control Board (INCB) for 2015–2017 to determine the global, regional, and national consumption of all controlled opioids, including anaesthetics, analgesics, antidiarrheals, opioid substitution therapies, and cough suppressants, in 214 countries and non-metropolitan territories.
Between 2015 and 2017, 90% of the world’s population consumed only 11% of controlled opioids (Richards et al. 2021). An average of 32 mg/person was consumed annually, but this was not equally distributed across the world (Figure 1). Consumption was the highest in Germany (480 mg/person), followed by Iceland (428 mg/person), the United States (398 mg/person), and Canada (333 mg/person). Oxycodone (35%) was the most heavily consumed controlled opioid globally, followed by morphine (15.9%), methadone (15.8%), and tilidine (14%).

Figure 1: Annual mean consumption of controlled opioids for 2015–2017 grouped by deciles for all countries and non-metropolitan territories (n = 214). Consumption refers to the total amount of controlled opioids distributed for medical purposes and excludes recreational use; it was calculated by determining the 3-year mean for 2015–2017 and dividing this by the 2016 population for each country obtained from the World Bank. Image published in the British Journal of Pain.
Key learnings
Disparities in accessing essential opioid medicines persist in most of the world. Consumption patterns should be monitored, and collaborative strategies should be developed to promote access and the appropriate prescribing of opioids in all countries and non-metropolitan territories.
This study was published in the British Journal of Pain. Retweet the summary of our findings here!
National use of prescribed opioids
We assessed trends and variation in opioid prescribing in primary care in England from 1998 to 2018 and factors associated with high-dose opioid prescribing by conducting a retrospective observational study using open data sources for all general practices in England.
We found a 34% increase in the prescribing of opioids between 1998 and 2018, but after correcting for strength, the increase was 127% (190 000 mg to 431 000 mg of oral morphine equivalency, OME, per 1000 population). There was also a 581% increase in the prescribing of high-dose opioids or 457% after correcting for strength (Curtis et al., 2019).
There was a range of prescribing behaviours across clinical commissioning groups in England over the latest 6-month in 2018 (March to August), with total OME differing almost eight-fold (Figure 2). If every practice in England prescribed high-dose opioids at the same rate as the lowest decile (0.17 items or £6.56 per 1000 patients per month) from March to August of 2018, we estimated that the NHS could have achieved a saving of £24.8 million.
A larger practice list size, ruralness, and deprivation were associated with greater high-dose prescribing rates.

Figure 2: Variation in opioid prescribing by clinical commissioning groups in England, March to August 2018, for total oral morphine equivalency (OME) for all opioid-containing preparations per 1000 registered patients. (from 52 700 mg to 416 000 mg per 1000 registered patients). Image published in Lancet Psychiatry.
Key learnings
Failing to account for opioid strength would substantially underestimate the true increase in opioid prescribing. Our findings support calls for greater action to promote best practice in chronic pain prescribing and reduce geographical variation. This study provides a model for monitoring opioid prescribing in primary and tools for practice and further research, which might help highlight areas where the action is most required and aid the targeting of interventions to reduce high-dose prescribing. Future work with patient-level data could reveal more detailed high-dose opioid prescribing patterns.
This study was published in The Lancet Psychiatry.
High-dose opioids
The risks of harm from opioids increase substantially at high doses, and high-dose prescribing has increased in primary care. However, little is known about what leads to high-dose prescribing, and studies exploring this have not been synthesised. We, therefore, conducted a systematic review of observational studies to assess factors associated with prescribing high-dose opioids in primary care.
We searched three databases and included studies that used patient-level primary care data and explored any factor(s) in people for whom opioids were prescribed, stratified by oral morphine equivalents (OME).
Six studies were included in our review, with a total of 4,248,119 participants taking opioids, of whom 3.6% were taking high doses (Richards et al. 2020). There were five factors associated with prescribing high-dose opioids in primary care, including the co-prescription of benzodiazepines, depression, visits to the emergency department, unemployment, and being male.
Key learnings
High doses of opioids are associated with greater risks of harm. Associated factors identify priority areas that should be considered when selecting, identifying, and managing people taking high-dose opioids in primary care. Coordinated strategies and services that promote the safe prescribing of opioids are needed.
This research was published in BMC Medicine and written about in The Conversation.
Over-the-counter (OTC) codeine
The patterns of opioids purchased over-the-counter (OTC) without a prescription are mostly unknown, and codeine is an opioid that is widely available OTC in many countries. We conducted a retrospective observational study using electronic point-of-sale data from IQVIA to assess national sales and public expenditure of OTC codeine-containing products purchased between 2013 and 2019 in 31 countries, including Argentina, Belgium, Brazil, Bulgaria, Canada, Croatia, Estonia, Finland, France, Germany, Greece, Ireland, Italy, Japan, Latvia, Lithuania, Mexico, The Netherlands, Poland, Portugal, Romania, Russia, Serbia, Slovakia, Slovenia, South Africa, Spain, Switzerland, Thailand, the UK, and the USA.
In six years, 31.5 billion units of codeine, costing £2.55 billion, were sold OTC in 31 countries (Richards et al., 2021). Total sales increased by 3%, and public expenditure doubled between April 2013 and March 2019. Sales were not equally distributed across the 31 countries; South Africa sold the most (31 units/person), followed by Ireland (24 units/person), France (16 units/person), Latvia (15 units/person), and the UK (11 units/person). The types of products (n=569) and formulations (n=12) sold varied.
Key learnings
In many parts of the world, substantial numbers of people may purchase and consume codeine from OTC products. Clinicians should ask patients about their use of OTC products, and public health measures are required to improve the collection of sales data and safety of such products, including the identification and prevention of codeine misuse and abuse and raising the awareness and education of the harms of codeine.
The findings are published in the journal Drug Safety.
We collaborated with Dr Tara Gomes and colleagues at the University of Toronto on a time series analysis of regulatory changes and rescheduling of low-dose codeine in Canada, published in CMAJ Open.
Essential Medicines Lists
Opioids are deemed essential medicines by the World Health Organization (WHO). However, many countries have inadequate access to them. Whether including opioids in national essential medicines lists (EMLs) influences national opioid consumption has not been evaluated. We conducted a cross-sectional study using the Global Essential Medicines Database to determine the numbers and types of opioids in 137 national Essential Medicines Lists (EMLs) and explore the relation of listing opioids in EMLs and opioids consumption.
The 20th edition of the WHO’s Model List of Essential Medicines included five opioids: codeine, fentanyl, loperamide, methadone, and morphine (Richards et al. 2020). Countries’ had a median of six opioids (IQR: 5–9 opioids) on their lists and the types (n=33) of opioids varied (Figure 3). Morphine (95%), fentanyl (83%), and codeine (69%) were the most commonly included opioids. After adjusting for country characteristics, there was no relation between mean opioid consumption and the number of opioids in EMLs.
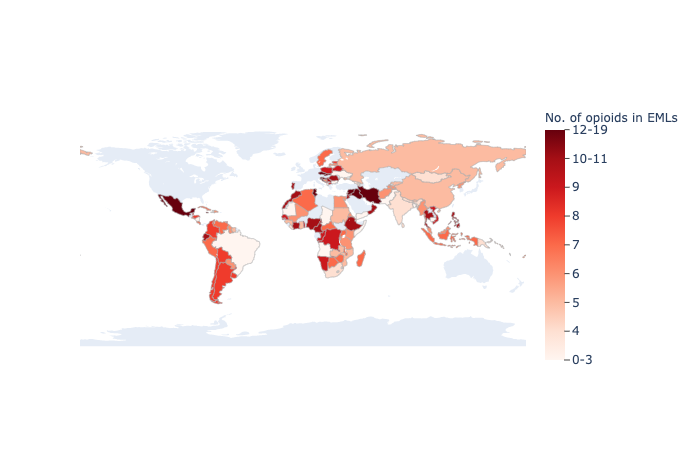
Figure 3: Number of opioids in national essential medicines lists (EMLs) grouped by nine quantiles. There were 137 countries with EMLs; countries in light grey did not have an EML. Image published in BMJ Global Health.
Key learnings
Simply putting an opioid in an EML may not increase supply or change prescribing habits. National EMLs should be regularly updated to reflect the availability of opioids and the populations’ needs for managing pain, palliative care, anaesthesia, and opioid dependence.
Tools and resources have been developed to improve the sharing of information regarding EMLs.
This study was published in BMJ Global Health and presented by Dr Richards at the inaugural Global Essential Medicines Meeting in Toronto, Canada. Retweet our Twitter post here!
The Oxford Catalogue of Opioids
The growing demand for analgesia, coupled with an increasing need to treat opioid dependence and overdose, has escalated the development of novel opioids. We searched seven databases systematically to quantify the number of opioid drugs developed and to catalogue them based on their pharmacology.
We included opioid drugs that targeted or had an effect or coeffect at one or more opioid receptors and extracted chemical and nonproprietary names, drug stems, molecular formulas, molecular weights, receptor targets, actions at opioid receptors and classes based on their origins to create the Oxford Catalogue of Opioids.
There were 233 opioid drugs identified, and ten unique drug stems with “fentanil” accounting for one-fifth of all opioids (Richards et al., 2021). Most (57%) drugs targeted mu-opioid receptors, and the majority (82%) were agonists at one or more receptors. Synthetic opioids were the most common (82%), followed by semisynthetic opioids (16%) and alkaloids (3%).
Key learnings
We created an online resource that detailing variations in opioid nomenclature, receptor targets, and actions. The Catalogue improves access to information for prescribers, regulators, researchers, and the public and promotes the safe use of opioids.
This work is published in the British Journal of Clinical Pharmacology. Retweet the summary of our findings here!
Concluding remarks
Disparities and variations in the use of and access to prescribed and non-prescribed opioids persist globally and nationally. While opioids can be overused or underused and can cause fatal and non-fatal harm, they still have a place in modern medicine in the right patient, at the right dosage regimen, and for the right reasons.
We developed several tools and resources, including measures on OpenPrescribing.net, improved access to data on essential medicines, and the Oxford Catalogue of Opioids. This research has also led to further research on deaths from opioids, the development of the Preventable Deaths Tracker, and a programme of research on preventable deaths; read more here: Preventable Deaths.
Dissemination
This research was examined for a Doctor of Philosophy at the University of Oxford, available for download. It has also been widely published in journals, including Lancet Psychiatry, BMC Medicine, BMJ Global Health, the British Journal of Clinical Pharmacology, and the British Journal of Pain, The Royal Society of Medicine Journal and BMJ Innovations.
The research has been presented at national and international conferences, and public engagement and scientific events. Blogs, news articles, podcasts, and social media have also been used to expand our reach.
In December 2022, Dr Georgia Richards also presented on surveillance and safety of pain medicines in the real world at the Cochrane PaPaS event at the Wellcome Trust. View this presentation on YouTube.
 Photograph of Dr Georgia Richards presenting this research on opioids at the National Institute for Health Research (NIHR) School for Primary Care Research (SPCR) Trainee Event at Pembroke College, University of Oxford in September 2019.
Photograph of Dr Georgia Richards presenting this research on opioids at the National Institute for Health Research (NIHR) School for Primary Care Research (SPCR) Trainee Event at Pembroke College, University of Oxford in September 2019.
Patient and Public Involvement and Engagement
In December 2019, we held a discussion group with three patients to receive input on the above studies, which helped shape what findings we emphasised, how we presented and displayed the results, implications discussed, and methods for dissemination.
 Photograph of the patient contributors providing input to this research on opioids, including Sean Jennings who had been taking opioids for 24 years and is now four years opioid-free.
Photograph of the patient contributors providing input to this research on opioids, including Sean Jennings who had been taking opioids for 24 years and is now four years opioid-free.
See more about Sean's story here.
Funding
Lead, Dr Georgia Richards, was supported by the National Institute for Health Research (NIHR) School of Primary Care Research (SPCR), the Rotary Foundation, and the Naji Foundation to conduct this research. A grant was obtained from the Primary Care Research Trust of Birmingham and Midlands Research Practices Consortium to purchase sales data on codeine from IQVIA. Article processing charges for open access publications were supported by the NIHR SPCR, the University of Oxford, the University of Toronto and the Li Ka Shing Knowledge Institute at St Michael’s Hospital. Travel to conferences was supported by grants from Kellogg College, Oxford, the NIHR SPCR, the Centre for Evidence-Based Medicine, Oxford’s Nuffield Department of Primary Care Health Sciences and the Canadian Institutes of Health Research, Ontario SPOR Support Unit, and St Michael's Hospital Foundation. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
References
-
Richards GC, Aronson JK, Mahtani KR, Heneghan C. 2021 “Global, regional, and national consumption of controlled opioids: a cross-sectional study of 214 countries and non-metropolitan territories”. British Journal of Pain.
-
Curtis, HJ. Crocker, R. Walker, AJ. Richards, GC. Quinlan, J. Goldacre, B. 2019 “Opioid prescribing trends and geographical variation in England 1998-2017: a retrospective database study.” Lancet Psychiatry, 6:2; pg140-150
-
Richards, G. 2018 “Making NHS data useful for GPs: OpenPrescribing at the RCGP Annual Conference 2018” NIHR SPCR blog.
-
Richards, G.C. Mahtani, K.R. Muthee, T.B. DeVito, N.J. Koshiaris, C. Aronson, J.K. Goldacre, B. Heneghan, C. 2020 “Factors associated with the prescribing of high-dose opioids in primary care: a systematic review and meta-analysis.” BMC Medicine. 18:68.
-
Richards, G. C. High-dose opioids – five factors that increase the risk of harm. The Conversation.
-
Richards, G.C. Aronson, J.K. MacKenna, B. Goldacre, B. Hobbs, R. Heneghan, C. 2021 “Sales of over-the-counter products containing codeine in 31 countries, 2013-2019: a retrospective observational study”. medRxiv, under peer review.
-
Boone, CG. Antoniou, T. Juurlink, DN. Rolf von den Baumen, T. Kitchen, S. Richards, GC. Tadrous, M. Gomes, T. 2021. “The impact of proposed regulatory changes and rescheduling on low-dose codeine purchasing in Canada: a time series analysis.” CMAJ Open (In Press).
-
Richards, GC. Aronson, JK. Heneghan, C. Mahtani, KR. Koshiaris, C. Persaud, N. 2020. “Relation between opioid consumption and inclusion of opioids in 137 national essential medicines lists.” BMJ Global Health.
-
Richards GC, Sitkowski, K. Heneghan C, Aronson JK. 2021. “The Oxford Catalogue of Opioids: a systematic synthesis of opioid drug names and their pharmacology”. British Journal of Clinical Pharmacology.
-
Richards, GC. 2019. “Treating post-operative pain? Avoid tramadol, long-acting opioid analgesics and long-term use.” BMJ Evidence-Based Medicine, 25:5.
-
Richards, GC, Lluka, LJ, Smith, MT, Haslam, C, Moore, B, O’Callaghan, J, Strong, J. 2018 “Effects of long-term opioid analgesics on cognitive performance and plasma cytokine concentrations in patients with chronic low back pain: a cross-sectional pilot study.” Pain Reports, 3:4 pe669.
-
Richards, G. 2018 “Opioids for pain: what’s the problem?” Centre for Evidence-Based Medicine blog.
-
Richards, G.C., Aronson, J.K., MacKenna, B. et al. 2022. Sales of Over-the-Counter Products Containing Codeine in 31 Countries, 2013–2019: A Retrospective Observational Study. Drug Saf. https://doi.org/10.1007/s40264-021-01143-2
-
Boone CG, Antoniou T, Juurlink DN, von den Baumen TR, Kitchen SA, Richards GC, Tadrous M, Gomes T. 2021. The impact of proposed regulatory changes and rescheduling on low-dose codeine purchasing in Canada: a time-series analysis. CMAJ Open. https://doi.org/10.9778/cmajo.20210173
Meet the team:
-
-
-
Ben Goldacre
Director of Bennett Institute for Applied Data Science, Bennett Professor of Evidence Based Medicine
-
Carl Heneghan
Professor of Evidence-Based Medicine



